

Background
Nodular lymphocyte predominant Hodgkin lymphoma (NLPHL) is a rare subtype of Hodgkin lymphoma (HL) with typically indolent clinical course. Although NLPHL is associated with favorable prognosis, late relapses, and a tendency to undergo transformation to aggressive lymphoma is seen in a substantial proportion of cases. Population-based long-term data on outcomes is limited.
Aims
We aimed to assess outcomes of the patients diagnosed with NLPHL in Finland.
Methods
We retrieved NLPHL patients diagnosed between 1995-2016 from the Finnish Cancer Registry (FCR) with complete follow-up to end of 2018. The Registry has an excellent coverage and provides accurate population-based nationwide data for all histologically verified cancers in Finland.
Gender and events such as histologically verified progression and transformation were obtained from the FCR. Date of death or emigration was verified from the Population Register and underlying cause of death (COD) from Statistics Finland. COD was categorized into three groups: lymphoma, solid cancer, or other cause. Patients were categorized into diagnostic calendar periods (1995-2002, 2003-2010, 2011-2016), gender, according to relapse, transformation, and patient status (alive, dead, emigrated) by end of 2018.
Standard descriptive statistical analyses were performed. Progression free survival (PFS) and all-cause overall survival (OS) was estimated via Kaplan-Meier method. Analysis of risk factors for OS and transformation was performed using the Cox proportional hazard model. Risk factors included diagnostic calendar period, age at diagnosis as a continuous variable (year), gender, relapse, and transformation. Multivariate analysis was performed including only factors with a p value < 0.05 from the univariate model. Two-tailed p-values < 0.05 were considered statistically significant. All statistical analyses were performed using R, version 4.0.2.
Results
We retrieved 414 patients with newly diagnosed NLPHL. Majority of the patients were males (n=320; 77%). Median age was 47 years (range 5 - 87), females being significantly older than males at diagnosis (59 vs 44 years; p < 0.001). We did not observe any statistically significant differences in age at diagnosis, gender distribution, progression, or transformation rates between the calendar periods.
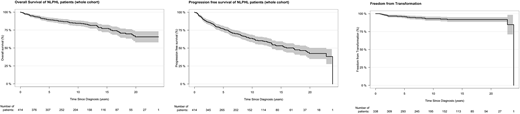
Five- and 10-year OS for the entire patient cohort were 89% and 84%, and 5- and 10-year PFS 77% and 64%, respectively (Fig. 1, 2). Eighty-six (21%) patients had at least one histologically verified progression (range 1 - 4). During the 11.1 years (range 0.7 - 23.9) follow-up, 81 (20%) patients died. The underlying COD was any lymphoma in 34 (42%), solid cancer in 14 (17%) and other cause in 33 (41%) patients.
Gender, age at diagnosis, and transformation were included in the multivariate model with respect to OS. Age at diagnosis (HR 1.07; 95% CI 1.05 - 1.09), and transformation (HR 2.6; 95% CI 1.5 - 4.7), but not gender, remained independent.
We found histologically verified transformation to large B cell lymphoma in 25 (7.4%) patients with ≥ 5-year follow-up from NLHPL diagnosis. Transformation was the first event in 15 (60%) patients, and 10 (40%) patients had one or more NLPHL progressions prior to transformation. The median age at the time of transformation was 57 years (range 20 - 87) and 17 (68%) of patients were males. The transformation free proportion over 5 years of follow-up was 96% and 93% over 10 years (Fig. 3). In multivariate analysis, gender, and age at diagnosis were not significantly associated with the risk of transformation. The 5-year OS after transformation was 50% which was significantly lower compared to the nontransformed patients with 5-year OS of 90%. Fourteen (56%) of the transformed patients died during follow-up, 13 from lymphoma and 1 from other cause.
Conclusion
In this large nationwide population-based study, females were 15 years older than males at the time of diagnosis. Twenty-five patients (7.4%) developed transformation to large B cell lymphoma. Age and transformation were independent risk factors for poor survival, whereas progression of NLPHL and gender were not associated with adverse outcome. We did not observe any survival difference between diagnostic calendar periods. Lymphoma was the main cause of death.
Malila:Cancer Society of Finland: Current Employment. Jyrkkio:Hospital District of Southwest Finland: Current Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal